


Introduction
The Great Barrier Reef, located off the east coast of northern Australia, is one of the world’s most popular marine tourism destinations. Stretching 2300 km along the Queensland coast, the reef incorporates approximately 3000 coral reefs, 600 continental islands and 300 coral cays1. The Australian Government Great Barrier Reef Marine Park Authority recorded 1.6 million full-day visitors in the 2018–2019 financial year, along with many more part-day and other visitation categories. The majority of these depart to visit the reef from Cairns in Far North Queensland2.
Medical emergencies are not uncommon among visitors to the Great Barrier Reef, and patients often require aeromedical retrieval due to the remote location3. Previous research has demonstrated that cardiac presentation(s) or cardiology service requirements make up a high proportion of retrieval cases3. There is little published data regarding the clinical characteristics of these patients.
This study sought to describe the characteristics and outcomes of patients who were retrieved to Cairns Hospital from locations along the northern Great Barrier Reef and were deemed to have a cardiac cause or a non-cardiac presentation with clinically significant cardiac involvement.
Methods
This observational study was a planned substudy of a broader analysis of medical retrievals from the Cairns/Cooktown section of the Great Barrier Reef, which lies between Mission Beach and Lizard Island. All patients who required medical retrieval from this section of the reef between July 2016 and January 2020 were eligible for inclusion.
The primary outcome was the proportion of all patients retrieved to Cairns Hospital who had a cardiac cause for presentation or cardiac diagnosis during their hospital stay. Secondary outcomes were the specific causes (diagnoses), investigation findings, management requirements and patient outcomes among this cohort, including the need for invasive coronary angiography (ICA) and percutaneous coronary intervention (PCI).
Retrieval data were collected from medical records maintained by LifeFlight Retrieval Medicine (Cairns base), which conducts most medical evacuations from northern Great Barrier Reef destinations in collaboration with Queensland Government emergency services and Retrieval Services Queensland. Given that the vast majority of patients retrieved are conveyed to Cairns Hospital, linked medical records from Cairns and Hinterland Health and Hospital Service were reviewed to collect data about final diagnoses, ECG results, cardiac troponin studies, ICA findings, requirement for PCI, and 30-day and 12-month mortality outcomes. Standard of care within Cairns Hospital is that all patients will have a final diagnosis made by a specialist, with the majority of patients with a cardiac diagnosis managed by a cardiologist.
Cairns Hospital is the major PCI referral centre for Far North Queensland. The cardiology department has two cardiac catheterisation laboratories, at which over 1500 ICA studies and over 500 PCIs were performed in 20204. Patient records and the Queensland Cardiac Outcomes Registry database were accessed to obtain ICA and PCI data.
All data were extracted using a purpose-designed data collection sheet, and then entered and analysed in a Microsoft Excel database. Descriptive statistics were reported, using frequency (n) and percentage (%).
Ethics approval
Ethics approval for the broader study was provided by the Far North Queensland Human Research Ethics Committee (reference LNR/2018/QCH/45008).
Results
During the study period, 120 patients were retrieved by LifeFlight Retrieval Medicine to Cairns Hospital. Of these, 46 (38.3%) were determined to have had a primary cardiac event or were allocated a cardiac diagnosis during their hospital stay. The mean age was 54 years (range 7–75 years), and 18 (39%) were female. Nine (20%) had a primary residential address in Australia.
Among all patients retrieved, 16.7% were determined clinically to have had a type 2 myocardial infarction (demand/perfusion mismatch or myocardial injury5). This suggests that the primary insult may have been non-cardiac, but resulted in subsequent cardiac involvement and requirement for cardiac investigation and or management.
After type 2 myocardial infarction, the most common diagnoses were primary arrhythmia (12.5% of all retrievals, making up 32.6% of total cardiac diagnoses), acute coronary syndrome (4.2% of all and 10.8% of cardiac diagnoses) and Takotsubo cardiomyopathy (3.3% of all and 8.7% of cardiac diagnoses). Acute heart failure accounted for 1.7% of retrievals and 4.3% of cardiac diagnoses.
Laboratory testing for cardiac troponin was positive in 36 (30.0%) of all patients retrieved and in 78% of those with a cardiac diagnosis. Of all the cases with a cardiac diagnosis, 14 patients (30.4%) died within 30 days of retrieval, all of which occurred during the index hospital admission. There were no further deaths after 30 days (12-month mortality also 30.4%).
There were 18 patients (15% of all retrievals) who underwent ICA, and four (3.3%) progressed to PCI. In addition to coronary angiography and intervention when required, guideline-directed medical therapy was initiated depending on the diagnosis. All patients requiring PCI survived to at least 12 months from their event.
Table 1: Primary and secondary outcomes – cardiac cause/presentations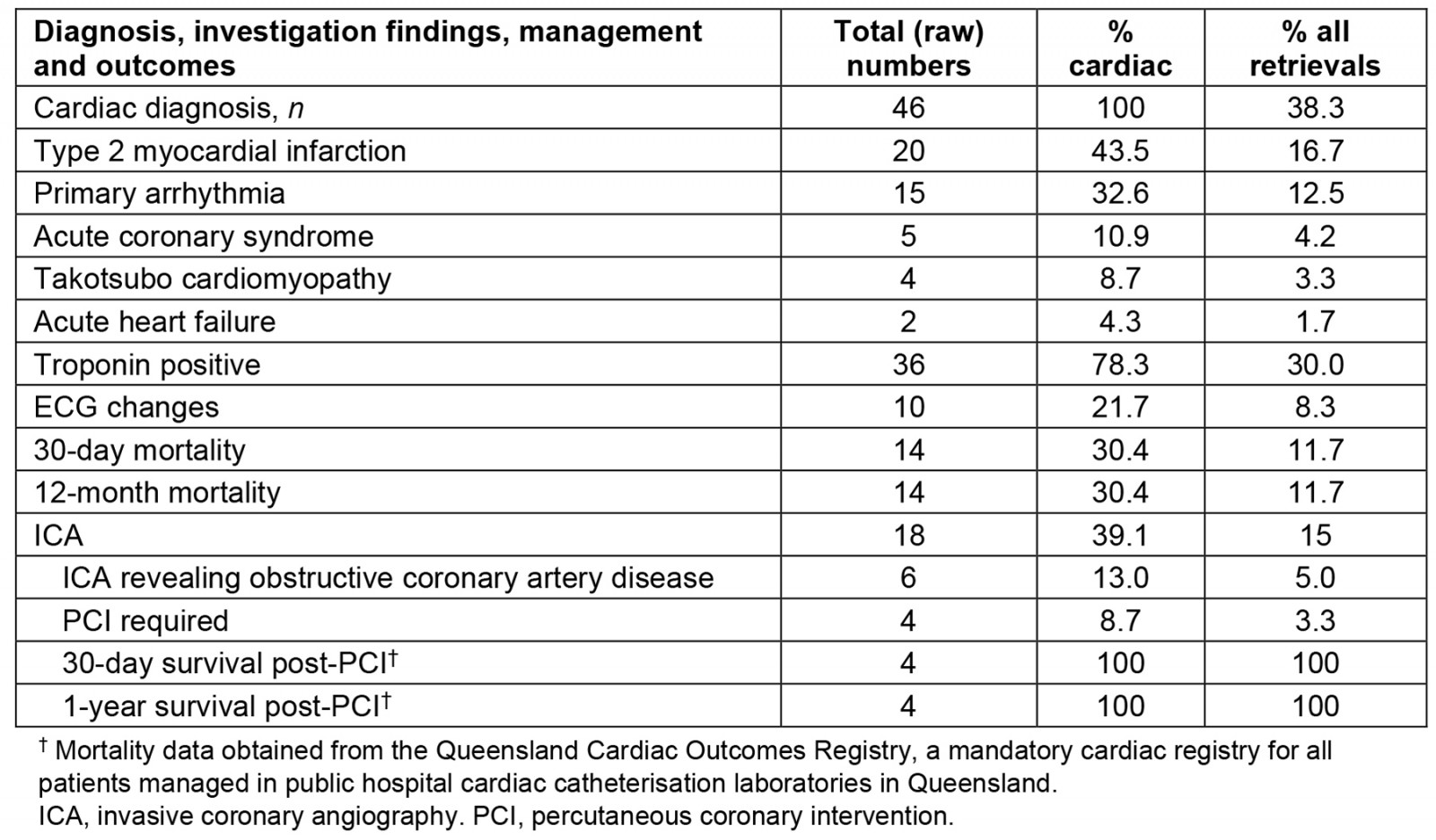
Discussion
This study demonstrates that cardiac-related presentations and diagnoses are common in patients retrieved from the Great Barrier Reef, accounting for just over one-third of retrievals. Of those with a cardiac presentation or diagnosis, approximately 39% required coronary angiographic assessment, of which 13% had obstructive coronary disease.
Outside of obstructive coronary disease requiring intervention, the cardiac catheterisation laboratory data confirm that a reasonable proportion of patients requiring retrieval presented with a non-coronary syndrome that can mimic a primary coronary cardiac event (such as Takotsubo cardiomyopathy or type 2 myocardial infarction). Takotsubo cardiomyopathy was first reported in the early 1990s and has since been accepted worldwide as an independent disease entity. It is characterised as elevation in cardiac troponin, transient hypokinesis of the left ventricular apex and is associated with emotional or physical stress (secondary to catecholaminergic surge) and often presents with chest pain or acute dyspnoea6.
Reef activities predominantly involve snorkelling, scuba diving, swimming and sailing1. Pre-hospital records suggested that a significant number of retrievals were precipitated by acute events related to these pursuits, such as drowning, possible envenomation and anxiety-provoking interactions with marine organisms. We hypothesise that these situations and exposures, particularly when they occur among tourists who are unfamiliar with the Great Barrier Reef, may account for the high proportion of Takotsubo cardiomyopathy and type 2 myocardial infarction relative to the published literature.
A number of articles in the literature have described ‘Takotsubo-like’ myocardial dysfunction findings on investigation of patients suffering immersion pulmonary oedema, a phenomenon that can occur while scuba diving, swimming or with ‘near-drowning’ events7-9. The clinical consequence, predicted recovery and prognostic implications from a cardiac perspective of these presentations is unclear7. A number of patients in the dataset were described to have had likely envenomation syndromes associated with their presentation. Envenomation events from jellyfish species are common in the waters of North Queensland, causing significant morbidity and occasional fatalities10. In particular, the venom from the Irukandji (Carukia barnesi) jellyfish native to the north-eastern waters of Australia, have been found to have significant cardiovascular system implications as part of the envenomation syndrome11,12. This is likely related to a catecholamine surge similar to the pathophysiology of Takotsubo cardiomyopathy12.
The primary limitation of this study is its retrospective nature. Additionally, data were confined to medical records maintained by LifeFlight Retrieval Medicine and Cairns and Hinterland Health and Hospital Service. A small number of patients may have been retrieved by other services, or presented to other health facilities. The findings are therefore limited to the Cairns region, and cannot be extrapolated to the southern Great Barrier Reef.
Of the cases retrieved and given a cardiac diagnosis, 14 (30.4%) died during their hospital admission, indicating the severity of cardiac conditions and cardiac complications from these events occurring on the Great Barrier Reef. A further limitation to the study is that a number of patients did not survive from reef retrieval to hospital to be formally assessed and receive a hospital-based diagnosis. A significant number of these patients may have suffered a cardiac event (such as a primary or secondary cardiac arrest) and died in transit. Given no definitive diagnosis was reached in these cases, the true burden of cardiac disease may in fact be higher (as a consequence of under-reporting).
Tourism service providers will benefit from this data, in part to educate their clients prior to embarking on trips to, and activities on, the Great Barrier Reef. It may also be useful in guiding the implementation of safety strategies, such as on-board automated external defibrillators, and essential training in basic life support for staff, to mitigate risk of such events occurring and improve rapid response strategies when they do. Automated external defibrillators have a strong evidence base and are a critical element in the chain of survival13.
Datasets such as these are also integral in assisting emergency services and recipient hospitals to efficiently and effectively manage patients requiring urgent retrieval from the Great Barrier Reef. These results will be useful in guiding protocols and equipment selection for retrieval services, and will assist clinicians involved in the emergency department evaluation of retrieved individuals.
Conclusion
Among patients requiring medical evacuation from the Cairns/Cooktown section of the Great Barrier Reef, a high proportion had a primary cardiac diagnosis. Further research is required to determine if recreational activities undertaken on the reef contribute to this burden of disease.
Acknowledgements
The authors would like to acknowledge the support LifeFlight Retrieval Medicine receives from the Queensland Government, Queensland Health, and Retrieval Services Queensland both as data custodian and tasking agency.
Funding
Tim Cahill received some funding from the Far North Queensland Hospital Foundation for data collection.
Conflicts of interest
All authors confirm there are no conflicts of interest.