



Introduction
Family planning programs encompass a spectrum of pivotal features, including a diverse array of high-quality counseling and family planning services, providing various methods of contraception, and receiving robust support from both commercial and government sectors. Although the emphasis on family planning has changed over time, the Family Planning Effort Index has consistently been a dependable source of information for development organizations and governments1. In low- and middle-income countries, approximately 371 million women of reproductive age (15–49 years) use contraception, thereby mitigating more than 141 million unintended pregnancies, 29 million unsafe abortions, and 150 000 maternal deaths in 20222. Contraception offers various health advantages for women and children, including reduced maternal mortality and improved infant survival rates, by allowing birth spacing and maintaining high nutritional status for both the mother and child3. Women’s educational attainment and higher use of contemporary contraceptive techniques are associated with accelerating fertility decrease4,5. Lower childbirth rates can create a demographic dividend by reducing dependence ratios, improving women’s labor-force participation, and encouraging resource investment. Education and family planning affect fertility, but contraception is a crucial predictor of it5. Cultural barriers, such as traditional preferences and desires for larger families and lineage, have been reported to hinder the adoption of family planning. These issues are especially prevalent in rural regions rather than developed cities and areas. These beliefs can influence the decisions of women and their spouses, negatively affecting the implementation of family planning services6. Between 2003 and 2010, decreased fertility rates were recorded in places with vital social programs and decent social circumstances, except Sub-Saharan Africa, which had the highest fertility rates7. From 2010 to 2015, the worldwide fertility rate for religiously unaffiliated groups was lower than for affiliated groups, which might contribute to beneficial long-term economic impacts due to lower youth dependence rates8,9.
Evidence-based research undertaken in Pakistan gives insight into the challenges that South-East Asian nations confront while using contemporary contraception, which include a lack of understanding, inadequate healthcare systems, and religious and cultural barriers10. The Pakistan Demographic and Health Survey (PDHS) 2012–1311 showed that 56% of married women of reproductive age wanted to use family planning services, but only 35% used them. Moreover, there was no improvement in the utilization of contraceptives as the prevalence of contraceptive use slightly decreased to 34% in PDHS 2017–1812. Furthermore, the prevalence of use varies depending on the geographical location, and the rural areas are commonly affected12,13.
Achieving the Sustainable Development Goal (SDG) target 3.7 of ‘universal access to sexual and reproductive healthcare services, including family planning, education, and information, and the incorporation of reproductive health into national plans and programs by 2030’ is crucial as the total contraceptive prevalence rate was 41.0%, according to the Pakistan Bureau of Statistics Annual Contraceptive Performance Report 2017–1814,15. Pakistan’s government and development organizations aim to accomplish equitable access to family planning services by 2030 as part of the SDGs by enhancing the availability and quality of family planning services, increasing awareness and education, and addressing cultural and social barriers. These endeavors are expected to support reproductive health outcomes and lower maternal and infant mortality rates in Pakistan16.
Comprehending the diversity of fertility patterns concerning couples’ family planning preferences and behaviors is crucial. This understanding can offer valuable insights into the determinants affecting impacting family planning decisions and facilitate the development of effective policies and programs to support couples in achieving their desired family size. The primary objective of this research is to examine the updated contraceptive method preferences of couples in rural and urban regions and how those translate to family planning practices among the different provinces. The research intends to assess the probability of contraceptive use based on demographic factors such as age, region, and education. The ultimate aim of this comprehensive analysis of the factors influencing contraceptive use and family planning behaviors is to inform policy decisions and enhance reproductive health outcomes.
Methods
Data source and study setting
The present study used secondary data from the Pakistan Maternal Mortality Survey (PMMS) 2018–1917, a specialized survey conducted as part of the PDHS. The PMMS was the fifth iteration of Demographic and Health Surveys carried out in Pakistan since 1990–91, emphasizing maternal mortality and its associated determinants. The unit of analysis for this research was women, and the dataset utilized was the PDHS ‘Individual Survey’ dataset (PKIQ7ASV). The ‘Individual Survey’ is part of eight other datasets included in the PMMS survey to provide well-grounded maternal health, mortality, and morbidity indicators that program developers and policymakers can utilize to evaluate and improve existing programs. The PDHS is a publicly accessible cross-sectional survey conducted in numerous countries by the National Institute of Population Studies, which is organized by ICF International, and the program is sponsored by the US Agency for International Development17,18. Data collection for the PDHSs comprises all provinces of the country and the merged areas Gilgit Baltistan, Azad Jammu and Kashmir through the stratified cluster sampling method. These regions are subdivided into rural and urban areas by selecting clusters from each stratum through probability sampling. This ensures a two-layer sampling strategy for selecting proportional samples from each region.
Primary outcome variable
The primary outcome variable was ‘Ever used contraceptives’ classified as a ‘Yes/No’ variable. Respondents who were currently using a contraceptive method were categorized as ‘Yes’; otherwise as ‘No’.
Independent variables
The independent variables include the respondent’s current age (organized into seven categories), type of residence (rural, urban), division (Punjab, Sindh, Khyber Pakhtunkhwa, Baluchistan, Gilgit Baltistan, Azad Jammu and Kashmir), education level (none, primary, secondary, or higher), and language of respondents (Urdu, Sindhi, Punjabi, Saraiki, Baluchi, Pushto, other).
Missing values
The dataset included a sample of 15 143 women from across Pakistan. Upon initial analysis, many missing values were removed, reducing the total sample size to 14 104. Previous articles published on missing values in data and how to deal with them have stated that bias is likely in analyses with more than 10% missing values19. Our sample’s total missing values were 6.86%, which is acceptable according to this criterion.
Data analysis
Descriptive frequencies and percentages were obtained to showcase the data based on sociodemographic variables, contraceptive use prevalence, and pregnancy-related factors. The phi coefficient χ² test (p>0.05, threshold 3) assessed the relationship between dependent and independent variables. Finally, multivariate logistic regression analysis was performed using age group, province, type of region, education level, and language as the independent variable categories to evaluate the likelihood of using contraceptives. The results were presented as the odds ratio (OR) with the corresponding 95% confidence interval (CI). We used Statistical Package for Social Sciences v27 (IBM Corp; https://www.ibm.com/products/spss-statistics) to perform our data analysis.
Ethics approval
Ethical approval for PDHS was granted from the National Bioethics Committee of Pakistan (4-87/NBC-346/19). Since this is a secondary analysis of the data, informed consent or ethical approval was not a prerequisite.
Results
Our sample consisted of 14 104 married women aged 15–49 years. The sample was proportionally divided between the provinces of Pakistan, with the majority of women belonging to Punjab (29.4%), followed by Sindh (19.6%), Khyber Pakhtunkhwa (19.5%), Baluchistan (12.3%), and a minor number from Gilgit Baltistan and Azad Jammu and Kashmir. More than half of the women (55%) belonged to rural areas, and an almost similar number (50%) had not received formal education; 60% of the women were aged less than 34 years. Table 1 describes the demographic characteristics of the sample in detail.
Regarding family planning, knowledge about contraception and the different methodologies was reasonably standard, with 88.2% of women claiming that they had heard of or at least knew one such method that could be used for the purpose. But when it came to practical application, the proportion is relatively low, with 51.7% of these women using or practicing any form of contraception. This information, when coupled with the fact that of the 87% of women in our sample who had given birth, 31.4% experienced at least one pregnancy loss during their lifetime, shows that the country is in a phase of high fertility and high infant mortality. Table 2 gives a picture of couples’ pregnancies and contraceptive practices. Information about couples’ willingness to conceive a child could not be drawn due to a significant amount of missing data.
Punjab province shows the highest contraceptive use (34.3%), whereas Baluchistan has the lowest (6.9%). The use of contraceptives in urban and rural populations is similar in all provinces except for Sindh and Gilgit Baltistan. In Sindh, 19% of the urban population uses contraceptives, whereas in the rural population, the proportion is 13%, but in Gilgit Baltistan, contraceptive prevalence is higher in rural (15.3%) than in urban (5.8%) areas.
In the provinces of Punjab and Sindh, contraceptive prevalence is 22.2% and 21.4% among women aged 25–29 years respectively. In Khyber Pakhtunkhwa, 21% of women aged 25–29 years use contraceptives, and in Baluchistan 22% of women aged 35–39 years use a contraceptive method. In urban and rural areas, women of aged 30–35 years who use contraception show a prevalence of 21% and 22% respectively. Using any contraceptive method among the age group 15–19 years is less prevalent than in any other group in all demographic regions.
Figure 1 shows the prevalence of contraception based on three categories: modern, traditional, and others. The modern category includes female sterilization, intrauterine device, male sterilization, injectables, implants, pills, condoms, standard days method, emergency contraception, and lactational amenorrhea method. In contrast, the traditional category includes rhythm method and withdrawal. Other categories include the utilization of multiple methods simultaneously. Specifically, the most preferred methods were condom (9.2%), injectables (6.2%), female sterilization (4.3%), pills (3.7%), intrauterine device (2.7%), emergency contraception (1.7%), and injectables and pills (1.3%), and 4.7 % of respondents used the traditional withdrawal method.
A χ² analysis was conducted to further explore the factors influencing contraceptive use among married women in our study sample, examining variables such as age group, education level, language spoken, childbirth history, place of residence, and region of residence. The analysis revealed significant associations between contraceptive use and several key demographic variables. Notably, age appears to strongly influence contraceptive practices, with a clear trend of increasing use as age advances. Childbirth history and region of residence also influence contraceptive use. Table 3 provides details of the analysis.
We performed logistic regression analysis to assess the likelihood of using contraceptives based on age group, province, type of region, education level, and language (Table 4). The regression analysis revealed that women aged 15–19 years were less likely (OR=0.71, 95%CI=0.51–1.01) to use contraception than the reference group. Residents of Gilgit Baltistan showed the highest likelihood (OR=3.32, 95%CI=1.54–7.13) of using contraceptives, followed by the Punjab division (OR=2.35, 95%CI=1.34–4.11). In contrast, the rest of the divisions – Sindh, Khyber Pakhtunkhwa, and Baluchistan – showed no significant results. The likelihood of contraceptive use was higher in urban areas (OR=1.53, 95%Cl=1.39–1.69). Noticeably, contraceptive use was less likely in women with no education (OR=0.63, 95%Cl=0.56–070) than in the other education levels. Language spoken showed no significant results when it came to contraceptives.
Table 1: Demographic characteristics of sample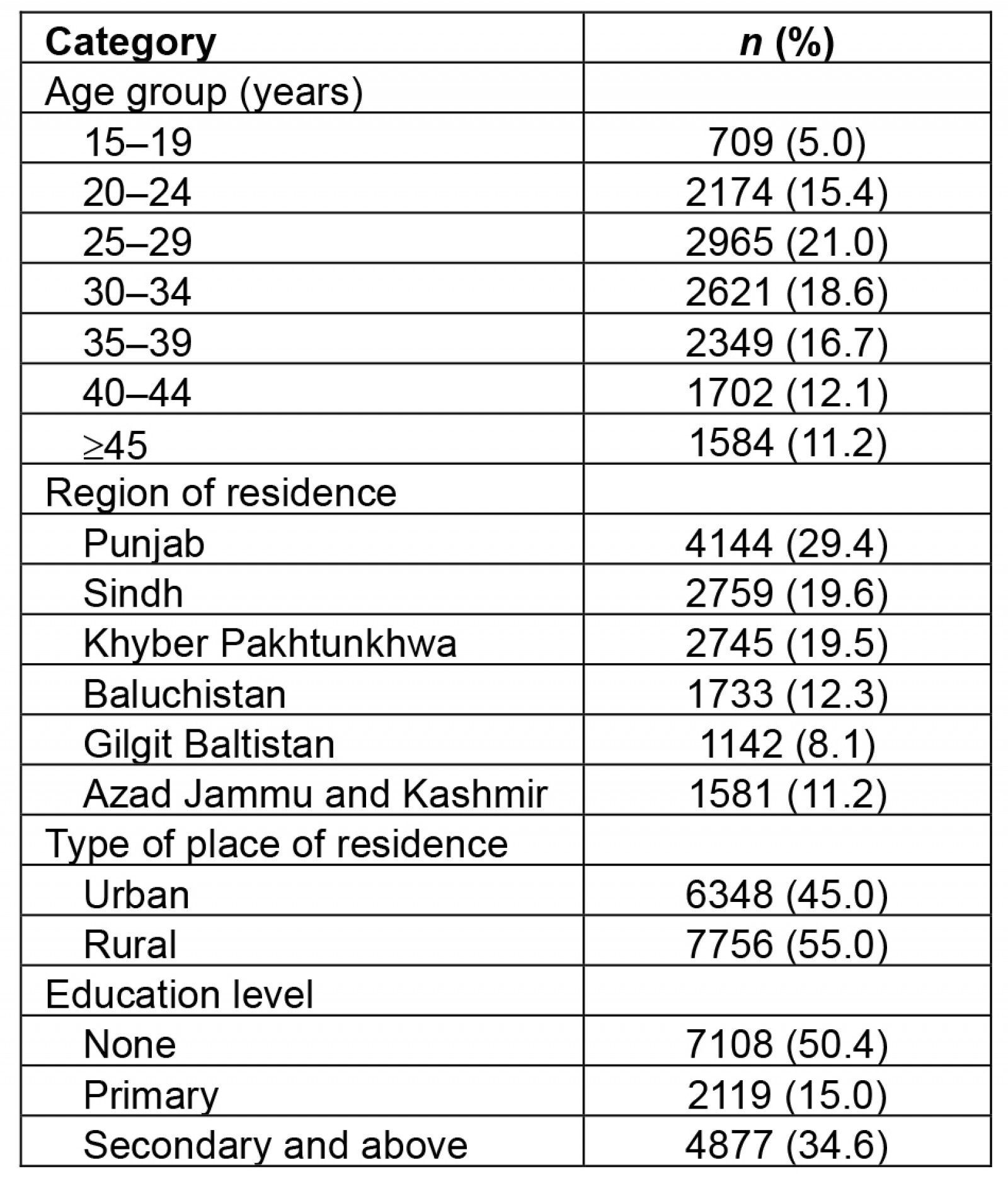
Table 2: Contraceptive awareness, use, birth, and pregnancy loss statistics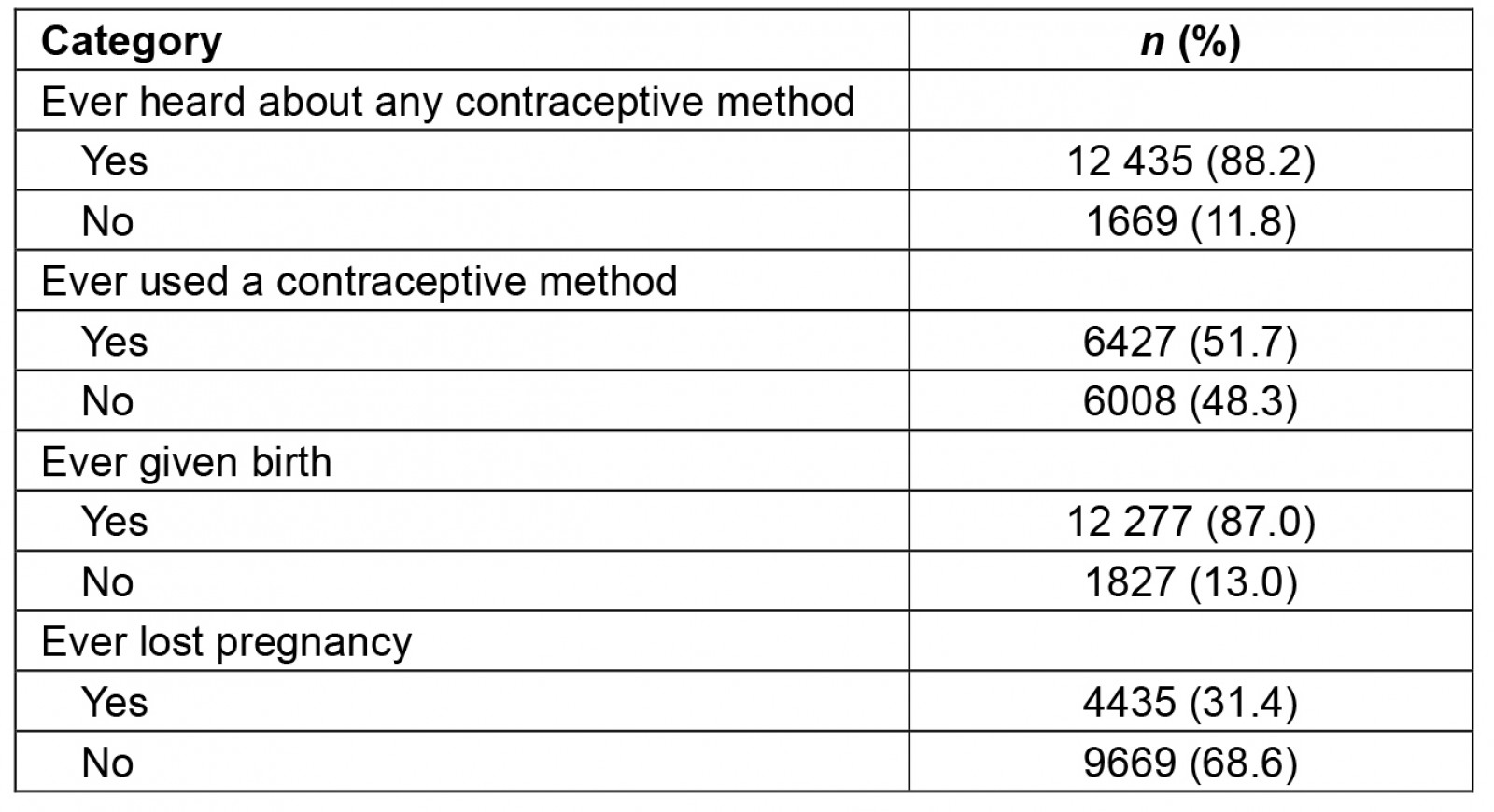
Table 3: Chi-squared analysis for contraceptive use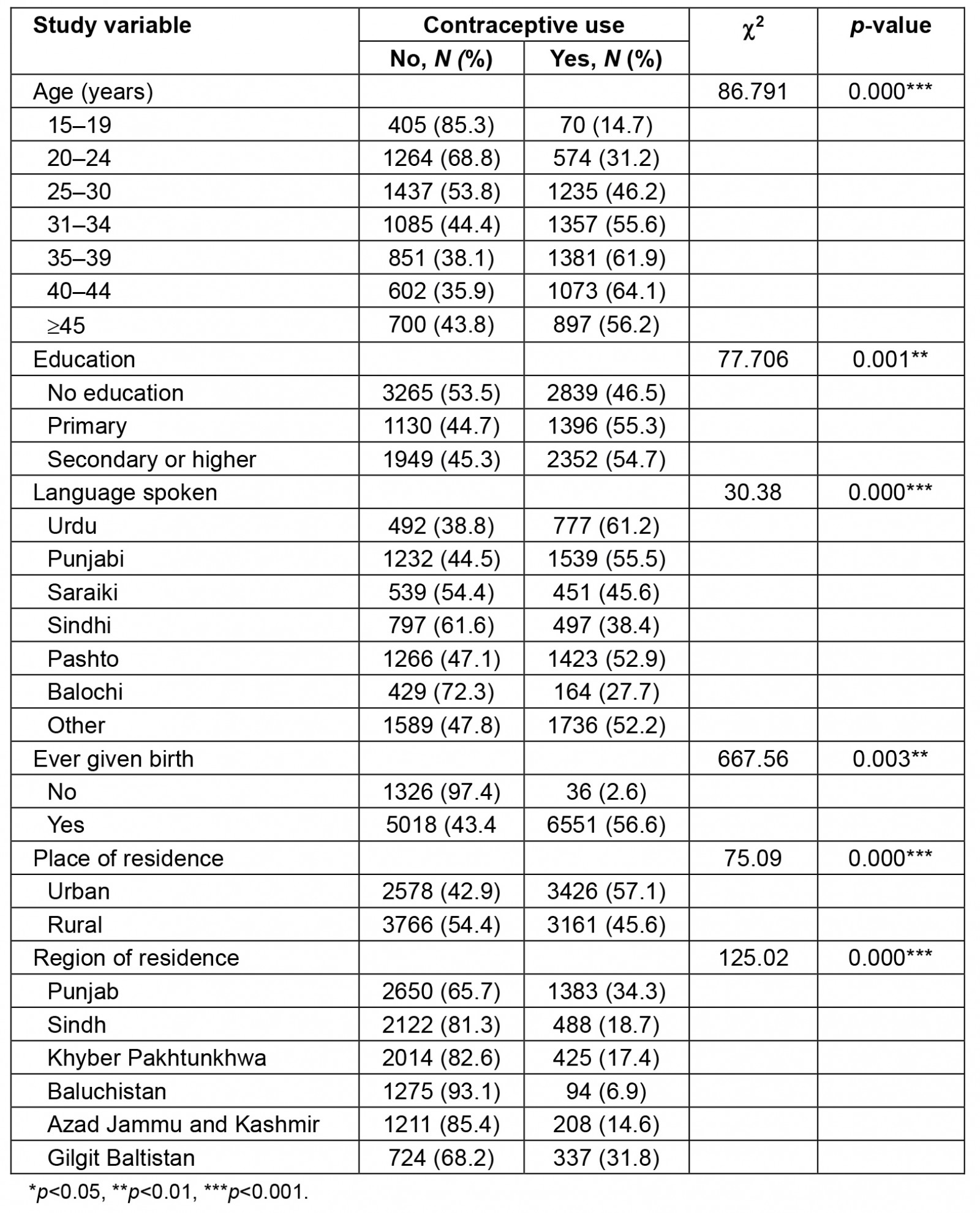
Table 4: Logistic regression analysis for use of contraceptive methods
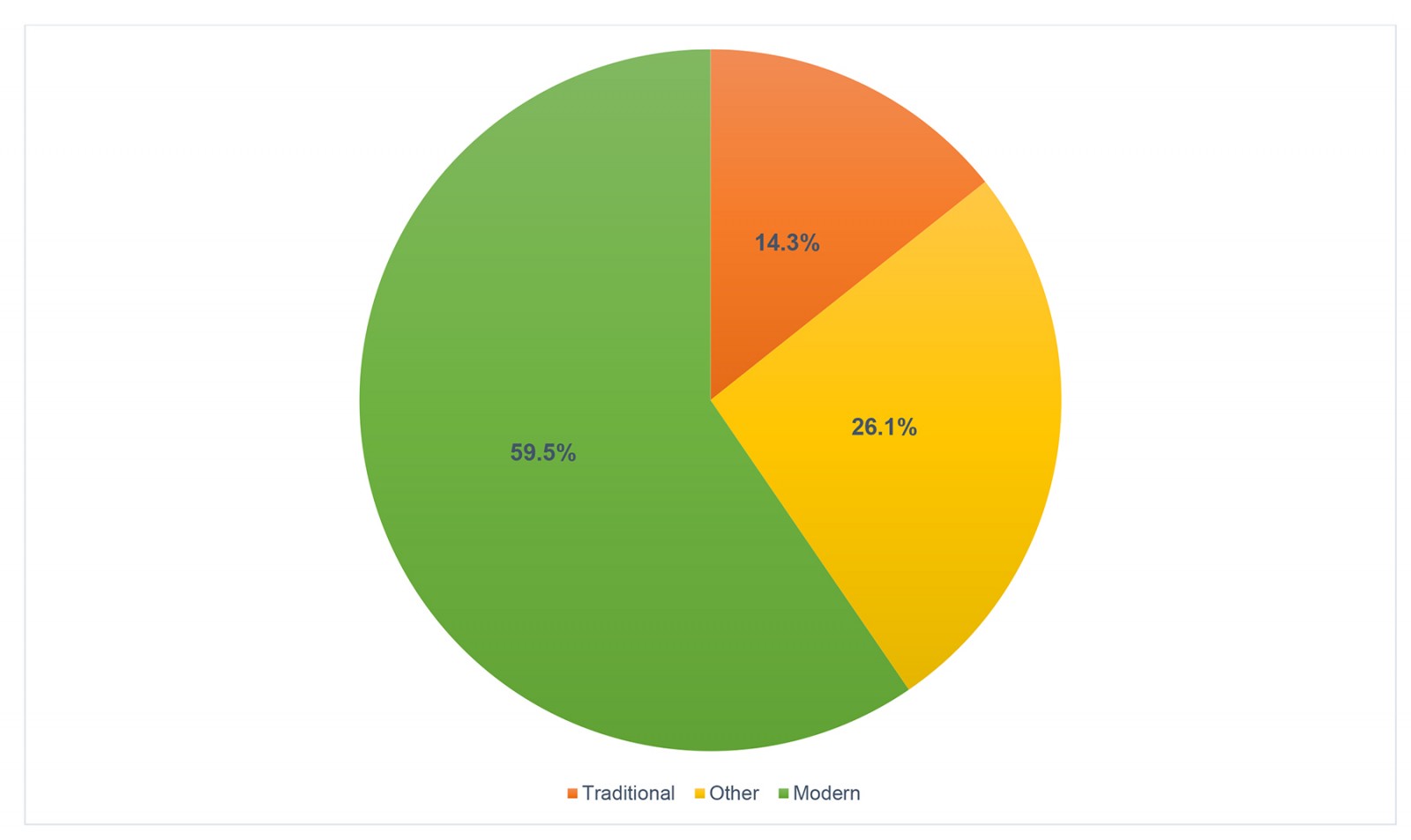 Figure 1: Categorical prevalence of contraceptive methods.
Figure 1: Categorical prevalence of contraceptive methods.
Discussion
The proactive approach of promoting reproductive health and planned conception is of paramount importance for the wellbeing of both children and mothers, mitigating the risks associated with infant and maternal mortality as well as risky abortions. It also aids in various non-health benefits such as empowering women, facilitating sustainable population growth, and fostering economic development in a nation20. Despite significant efforts by the government of Pakistan to implement family planning initiatives, the PDHS 2019 shows that there is a considerable disparity as well as low prevalence of contraceptive use among inter-division and urban–rural areas of Pakistan, regardless of the high unmet need for contraception17.
This current study elucidates that a considerable proportion of women heard about contraceptive methods. However, less than half of the women had ever used contraceptive methods, which aligns with the findings of Meherali et al20, where contraceptive use was only 30% among women of childbearing age who have been married at least onceClick or tap here to enter text.. According to the findings of Mustafa et al21, the most probable reasons for hesitancy towards the use of contraceptive methods could be low awareness about contraceptive methods, lack of availability of high-quality services, side effects, incomplete family size, negative attitudes, disapproval from family members, and religious considerationsClick or tap here to enter text..
Despite being a developing country, Pakistan faces significant challenges related to unintended pregnancies, miscarriages, and stillbirths, as evidenced by a community-based study indicating a high rate of stillbirths of 33.6 per 1000 total births22. Similarly, a considerable proportion of women in this study experienced pregnancy loss. Moreover, more than three-quarters of the women who participated in the survey had given birth. According to the 2020 Pakistan Demographic Survey, Pakistan’s fertility rate is 3.7, above the replacement level23. High fertility rates can negatively affect the health sector, economic development, and educational systems of the country and hinder women’s empowerment9Click or tap here to enter text.. Several studies have demonstrated a relationship between reduced pregnancy loss and the use of contraception in many countries. Increased use of contraceptives contributes to the reduction of the number of births, which in turn reduces maternal mortality, stillbirths, and child mortality24,25.
The majority of the participants in this study used condoms as a modern contraceptive method followed by injectables. Similarly, Meherali et al20 reported that the most commonly employed contraceptive method was condoms (30.5%), whereas MacQuarrie et al26 found a lower use of condoms (10%). As per Meherali et al, a high rate of contraceptive use was recorded in Punjab (35.2%) compared to other provinces. The potential influencing factors for increased contraceptive use in Punjab could include enhanced outreach services provided by female health workers, improved use of antenatal care facilities, well-organized family planning services, a higher female literacy rate, and a more significant number of economically active women in Punjab in comparison to other regions of Pakistan17,27.
Women aged 35–39 years showed a higher likelihood of using contraception than those aged 15–19 years, especially women in urban areas and those with educational attainment. The lack of proper awareness, financial constraints, long-distance commutes, and limited availability of transportation are the common hurdles to seeking healthcare facilities among rural women20,21. Additionally, rural-dwelling women show a greater propensity for experiencing unmet family planning needs than their urban counterparts, particularly among those with limited exposure to mass media and experiencing unemployment and apprehensions regarding contraceptive side effects17. Conversely, healthcare infrastructure, the availability of reproductive health services and education among women in urban areas are far better than in rural areas, which could contribute to increased use contraceptive measures among urban women28. Numerous studies show that the use of contraception is more prevalent among older women than in aged 15–24 years. A greater tendency towards using family planning methods was observed among women with three or more children than those with fewer children. Moreover, newly married women are typically supervised by their spouse or mother-in-law, who holds the ultimate decision-making authority. However, women’s autonomy in making choices increases as they get older28,29.
The logistic regression in this study indicates that residents of Gilgit Baltistan showed the highest probability of using contraceptives, followed by the Punjab division. This regional disparity was also evident in another study, where women residing in Gilgit Baltistan exhibited an increased relative risk in the use of condoms and intrauterine devices. Also, they are more inclined to use injectables. On the contrary, the regions of Punjab and Azad Jammu and Kashmir demonstrate substantially diminished adjusted risks associated with ingesting oral contraceptive tablets26. There was no association between the language spoken and the use of contraception. Contrary to this finding, Khan et al30 identified a considerable impact of language among Baluchi, Sindhi, Saraiki, and other Urdu languages. The use of contraception methods was more common among women who speak the Saraiki language than among women who speak Urdu. However, Punjabi and Pushto speakers showed no differences.
The findings in this study yield major perspectives into the current status of contraceptive use in Pakistan, which is relevant to understanding the health and wellbeing of the population. Despite the PDHS being a valuable tool for policymakers, government, and private organizations, the self-reported data are susceptible to recall bias, a notable limitation. Furthermore, the cross-sectional survey design was unable to articulate a causal connection between outcomes and other contributing factors, such as sociocultural beliefs related to contraceptive use and the influence of family members. Extensive research to identify the underlying factors contributing to the low prevalence of contraceptive use among women in Pakistan is necessary to tackle barriers to contraceptive use.
A multifaceted approach is needed to address the issue of low contraceptive use in Pakistan, which includes the prioritization of high-quality education, advocacy of government policies, involvement of multiple stakeholders, comprehensive counseling, equitable access to contraception, and promotion of women’s empowerment, as well as public awareness to tackle the stigma associated with contraception, which is crucial in the context of family planning, especially in marginalized areas. Both men and women should be equally educated without inter-division or urban–rural disparity to understand the importance of family planning and its associated health benefits.
Conclusion
Our study investigated the contraception and family planning trends among the Pakistani population. The results highlighted an increasing prevalence of contraceptive use with age, particularly in the group of 35–39 years when compared with that of 15–19 years. Although the majority of the participants had heard about the use of contraception, the practical application was nowhere near that. Inequalities in use were evident as the prevalence of contraception use was higher in urban areas than in rural areas and between the provinces: Punjab showed the highest use of contraception and Baluchistan showed the lowest. Also of note, contraception use was lower among those who did not receive formal education as than among participants with higher levels of education.
Overall, the study emphasizes the need to implement focused educational initiatives and counseling interventions with an integrated approach to enhance women’s empowerment and their pivotal role in making decisions pertinent to family planning. It is also imperative to prioritize accessibility and affordability of contraceptive methods while paying meticulous attention to target women in lower socioeconomic regions.
Funding
No funding was received for this research.
Conflicts of interest
The authors declare no conflict of interest.